Nerves are formed by the axons of nerve cells (the axon is an extension of the nerve cell). These axons are or are not surrounded by myelin sheath from other cells: Schawnn cells.
Anatomy:
A nerve is made up of different elements:
- Axon
The axon is a nerve fiber that originates from the cell body of the neuron and varies in length depending on the cell from 1mm to over 1m.
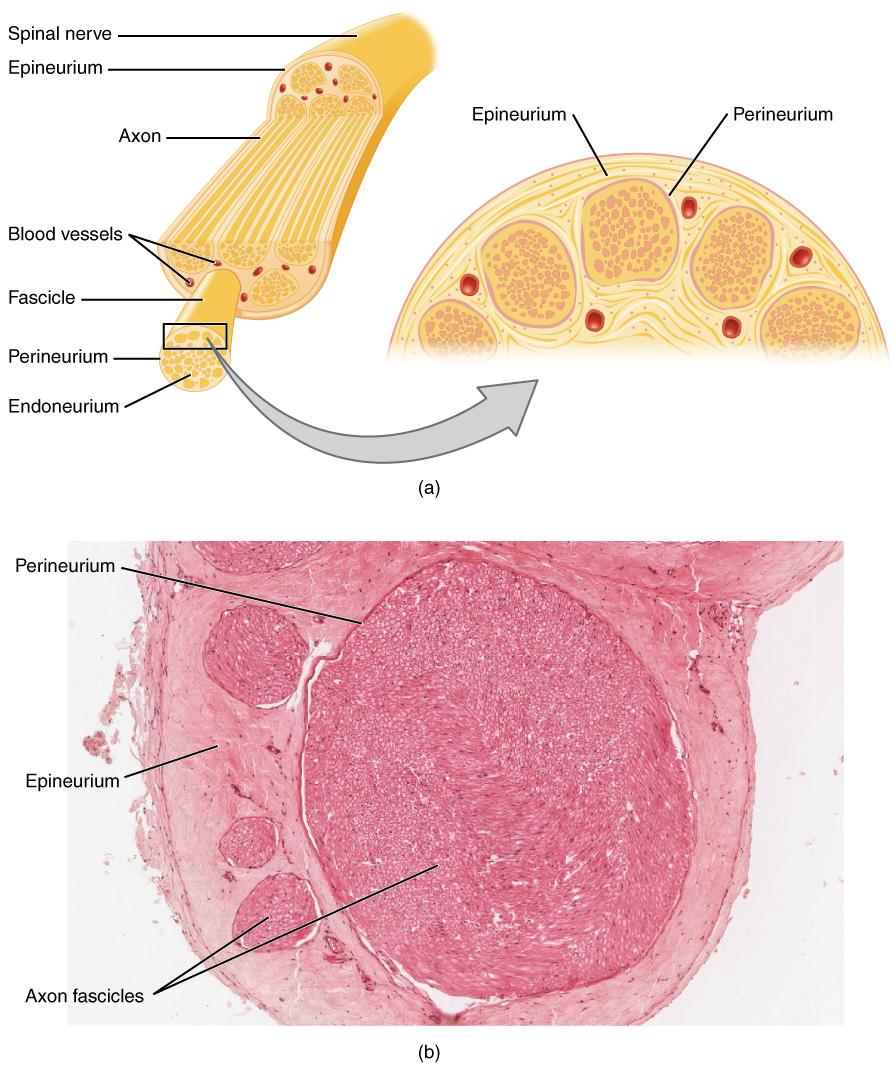
- Endoneurium
The endoneurium is the innermost or deepest layer of connective tissue comprised within a peripheral nerve.
- Perineurium
Each fascicle is surrounded by a sheath, the perineurium.
- Epineurium is a loose connective tissue, is subdivided into two layers, internal and external. The inner Epineurium is a loose connective tissue
- The mesoneurium is the outermost tissue surrounding the peripheral nerve trunks.

Nerves can be classified according to their size:
Name Diameter Conduction Velocity Role
A alpha 13-30 µm 80-120 m/s Proprioception (motor skills)
A béta 6-12 µm 35-75 m/s Sensitivity
A delta 1-5 µm 5-35 m/s Pain. Temperature
C 0,2-1,5 µm 0,5-2 m/s Pain. Temperature
The A alpha, A beta and A delta fibers or nerves have a myelin sheath, the C fibers do not.
They can be classified by their functions:
Efferent fibers carry information from the center to the periphery.
Afferent fibers carry information from the periphery to the center.
Efferent fibers are composed of:
- Somatic motor nerves that innervate the striate musculature (motor muscle).
The striated muscle is the muscle of movement: the biceps, for example, which allows you to bend your arm or the calf which allows you to stand on tiptoe or press the pedal of the bicycle. - Nerves of the vegetative system which innervate the smooth muscles (in particular in the intestines), the heart and certain glands.
Afferent fibers carry sensory information. They are composed of:
- Myelinated fibers for tactile sensitivity (touch), proprioceptive (position of a joint, length of a muscle), some painful and thermal information.
- Unmyelinated fibers for pain and temperature.
Afferent fibers carry information from more or less specialized receptors:
- Sensory receptors: mechanoceptors sensitive to pressure (corpuscles of Pacini, Ruffini, Meissner, Merkel cells) and the stretching of the skin, chemoreceptors for taste and olfaction and finally teleceptors for vision,
- Proprioceptors: measures pressure and tension in muscles, joints and tendons (Golgi tendon organ, Pacini corpuscle, Ruffini corpuscle),
- Interoceptors: modified by modifications of the internal environment (baroreceptors, chemoreceptors)
- Nociceptors: polymodal (several types of stimuli) or specific.
The vegetative system is composed of the orthosympathetic system and the parasympathetic system. these two systems are, in general, antagonists and take care of the innervation of the deep organs (heart, stomach, intestine, sweat of the skin,…)
Composition of a nerve:
The afferent and efferent fibers join to form mixed (sensitivomotor) nerves, sciatic nerve for example.
The efferent fibers alone form a motor nerve (facial nerve for example).
The afferent fibers alone form a sensory nerve (trigeminal nerve for example).
Pathology: Peripheral neuropathies.
The different attacks are described according to whether or not the axon is affected, whether or not the myelin sheath is affected,
The achievement of an efferent nerve gives paralysis or paresis.
Involvement of an afferent nerve leads to disturbances in superficial (touch) and/or deep (proprioception) sensitivity.
Involvement of the autonomic nervous system gives rise to a dysautonomic syndrome.
Isolated involvement of small A delta and C fibers results in small fiber neuropathy.
Functional exploration: Electrofisiological examinations.
The nerve has the property of conducting nerve impulses. The application of an electric current to its level causes the formation of an action potential. Collecting the nerve potential (sum of the action potentials) at a distance from the stimulation is the basis of the technique for measuring motor and/or sensory conduction velocities.
Motor conduction is measured after stimulation at the level of the muscles, it is the motor response.
Sensory conduction is measured by stimulating the nerve and collecting a nerve potential (sum of nerve action potentials).
These are sometimes unpleasant or even painful, patients should be warned.
The different exams available are:
- Electromyogram by nerve stimulation and also collection of spontaneous or voluntary muscle activity.
- Somatosensory evoked potentials by cutaneous stimulation with collection of the response remotely along the path of the nerve or at the level of the skull.
- Motor evoked potentials by transcranial magnetic stimulation at the level of the motor cortex and collection of the response at the muscular level.
These different examinations make it possible to define neurological damage by differentiating between damage to the axon (axonopathies) or myelin (myelinopathies).
Axonopathies
In the event of an acute attack, for example a trauma, there are 3 stages of nerve damage:
- Neupraxia corresponds to an isolated impairment of the myelin sheath,
- Axonotmesis corresponds to an axonal attack without interruption of continuity,
- Neurotmesis corresponds to the rupture of continuity of the nerve.
In the case of chronic damage, there is little slowing down of nerve conduction velocity but a reduction in amplitude by reduction in the number of functional axons. This reduction is length dependent: the further away from the central nervous system the greater the loss (see small fiber neuropathy and acute polyradiculoneuritis development).
Myelinopathies
The disappearance or impairment of the myelin sheath leads to a marked decrease in conduction velocities during electrophysiological examinations.