Myofascial syndrome of the gluteus minimus muscle is responsible for pseudo-sciatica.
The contracture of this muscle is responsible for pain projecting on the lateral part of the thigh sometimes up to the ankle (red zone).
In general the pain does not go down in the foot. Typical sciatic pain is more posterior but confusion is often common…
The pain is increased by prolonged standing, trampling, the sitting position is quickly uncomfortable with a permanent need to change position.
This type of pain fluctuates throughout the day with a clear tendency to worsen as the day progresses and decreases during the night.
The usual analgesic treatments have little or no effect on this pain.
The origin of this muscle contracture is, most of the time, postural.
It can be related to:
- lower limb length asymmetry,
- a static problem of the pelvis (damage to the sacroiliac joint),
- lameness in a post-traumatic foot, ankle, knee or hip or post-operative context (hip prosthesis, knee prosthesis, etc.),
- an asymmetrical muscular work overload (for example worker carrying heavy equipment always on the same side).
Diagnostic
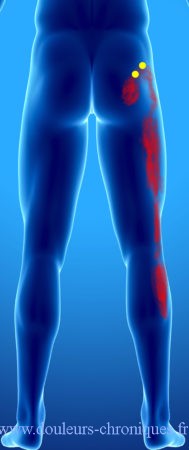
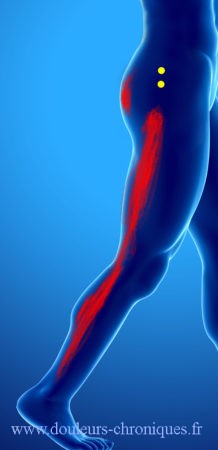
Strong palpation of the area between the iliac crest and the greater trochanter (hip bone on the side) is very painful and reproduces pain in the entire lower limb (green area).
If in doubt, an injection of local anesthetic into the painful muscle makes the pain disappear in the underlying limb.
In the event of a positive diagnosis, a cause must be sought:
- Weight-bearing pelvic X-ray looking for lower limb length inequality.
- A consultation with an osteopath to check the proper functioning of the sacroiliac joints.
- A consultation with a podiatrist for possible corrective insoles.
Treatment
- The treatment of another pain in the lower limb responsible for lameness.
- The treatment is based on physiotherapy with deep muscle massage and if possible ischemic compression followed by stretching.
- At home, compression for ten minutes every day with a tennis ball, which is rolled slowly over the muscle with its own weight on the ground, is particularly effective. Stretching exercises should follow this self-massage. In the event of prolonged standing, it is advisable to raise the feet 5 to 10 cm alternately (for example with a foot callus). It is also advisable, in people sleeping on the side, to block the knees with a cushion or a pillow during the night (cushion between the knees).