Anatomical reminder
Description
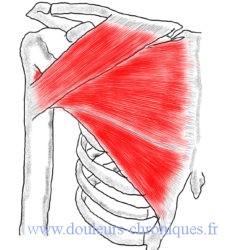
Made up of the pectoral muscle which has 3 heads:
- Head Clavicular
- Sternal head
- costal leader
- An abdominal boss for some
and subclavian muscle
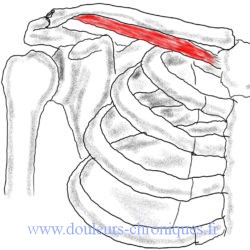
- The subclavian muscle sits under the collarbone and covers the first rib. It inserts into its medial part on the junction of the first rib and its cartilage. Laterally, on the underside of the clavicle.
- The pectoral muscle is inserted laterally on the greater tubercle of the humerus, in two layers. Medially, the muscle inserts into four separate parts:
- Clavicular fibers
- The sternal fibers
- The costal fibers from the 2nd to the 6th or 7th rib.
- The abdominal fibers on the aponeuroses of the rectus and external oblique muscles of the abdomen
Functions
- Adduction of the arm at the shoulder (lower arm position)
- Shoulder arm abduction (top)
- Anterior displacement of the humeral head
- Internal arm rotation
- Anterior elevation of the arm up to approximately 100° upwards
Myofascial syndrome of the pectoral muscle
Description
The subclavian muscle


Note that the referred pain of the subclavian muscle descends from the clavicle to the hand to the ipsilateral hand by jumping elbow and wrist
The pectoral muscle
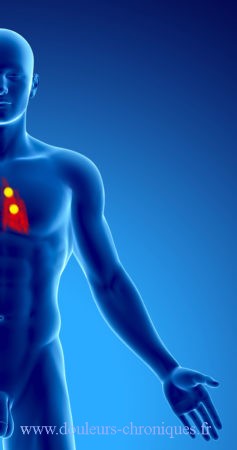



Depending on the affected part of the muscle, different referred painful territories are described (see overlying diagram). This pain can be associated with visceral effects, mainly cardiac:
- tachycardia, ventricular extrasystole (trigger point between the 5th and 6th rib)
- Association between myocardial ischemia and pectoral muscle pain
Diagnostic
Palpation of the muscle finds painful areas, the examination will be sensitized by abduction of the arm at 90°. The area responsible for heart rhythm disturbances is on the right side between ribs 5 and 6 to the right of the xiphoid.
There is little limitation of movement related to the attack of this muscle.
Triggering factors
- Lifting heavy objects, especially with arms stretched forward
- Repeated shoulder abduction
- arm immobilized in adduction (sling, against sling)
- Round shoulder position (shoulder forward favored by certain activities such as masonry, carer, tennis, judo, gardening and hedge trimming, etc.)
Treatment
- Passive stretching of the muscle by arm abduction in partial or total extension associated with external rotation
- Infiltration of lidocaine in painful areas followed by stretching
- A particularity of this treatment is based on teaching the patient to differentiate between muscular pain and pain of cardiac origin. Indeed the patient, if he thinks of heart pain, stops all physical activity, which is totally counterproductive in the management of his pain and his health in general. The demonstration of the triggering of his pain by palpation is therefore essential for his future management.
- In standing position, it is necessary to correct the patient postures bent forward. In women, wearing high heels can help correct posture. In men and women, a change of foot support from the heel to the front of the foot often makes it possible to significantly improve the situation.
- In a seated position, a lumbar support is necessary, changing the statics of the upper body and allowing the anterior projection of the shoulders to be reduced. Similarly, the back of a seat at work or on a sofa must be tilted by about twenty degrees to avoid anterior projection of the shoulders.
- At night the pillow should not elevate the shoulder in the supine position. In lateral decubitus a pillow under the elbow helps to avoid a deleterious shortening of the muscle.
- Finally self-stretching, carried out in the frame of an arm door between 90° and 180°, by pressing on the amount of this door (open), while advancing forwards must be repeated every day.