Part of the underlying descriptions are taken from Robert Maigne’s book: “Pain of spinal origin, understanding diagnosis and treatment”
All of the elements making up the mobile spinal segments can be responsible for acute or chronic low back pain:
- the intervertebral disc
- the posterior joints
- the ligaments
- muscles
Chronic forms
Low back disc pain
The role of the disc in chronic low back pain was considered essential. However, many pains result from a more complex mechanism, the disc injury leading to abnormalities in the functioning of the posterior joints and the interspinous ligaments. it is therefore appropriate to distinguish:
- Low back disc pain in which the disc lesion is directly responsible for the pain
- Low back pain due to segmental instability of which the disc lesion is the cause but the pain is linked to the dysfunction of the posterior joints and/or the interspinous ligament.
Low back pain can come from:
- the superficial fibers of the annulus and the posterior common ligament
- the inter-apophyseal joint (posterior joint)
- the interspinous ligament.
The disc injury is directly responsible for the pain
The clinical consequences of this pathology are:
- The patient presents with more or less spaced episodes of acute low back pain.
- Lower back pain is episodic or permanent and is increased by coughing, sneezing, sudden straining, defecation, straining
- Some positions are untenable, others completely relieve the patient
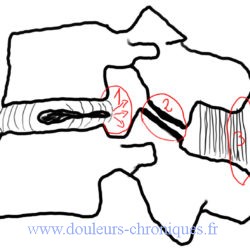
The disc injury is indirectly responsible for the pain
Initially, the cartilaginous and disc damage is responsible for an antero-posterior vertebral slippage with an impact on the posterior joints. Secondly, excessive twisting leads to posterior joint damage on one side and the appearance of a herniated disc on the other with a narrowing of the lumbar canal.
It will be noted that:
- often, it is the posterior joint pain that predominates at first.
- there is no parallel between the radiological images and the intensity of the low back pain.
- at the beginning of the pathology there is instability of the spinal segment
- The evolution is towards fixation of the segment by fibrosis and osteophytosis.
Lower lumbar posterior joint back pain
Segmental instability caused by disc damage often leads to pain related to the posterior joints.
This posterior joint pain causes lower back pain but also pain radiating towards the buttock and lower limb.
The clinical characteristics of this pain are:
- a lack of worsening of pain when coughing, sneezing or defecating
- pain increased by sitting.
- absence of pain during trunk flexion and straightening
- any increase in lumbar lordosis increases pain: lying position with increased lordosis (in contradiction with the description of R. Maigne)
- A very significant sign in our opinion is pain upon pressure from the thumb of the affected vertebral segment during retroflexion of the trunk in a standing position.
In this case the diagnosis and treatment will be confirmed by infiltration of the posterior joints in question with a mixture of local anesthesia and corticosteroids. These injections provide relief for a few weeks to a few months which will allow rehabilitation to be carried out with strengthening of the lumbar and abdominal belt.
Some practitioners offer posterior joint rhizolysis using thermo coagulation. This technique is interesting but the long-term results are disappointing. They must be accompanied by active rehabilitation aimed at controlling lumbar hyperlordosis and thereby reducing the pressure exerted on these joints.
Low back pain of ligamentous origin
The origin of the pain is sometimes, even often, of ligamentous origin, particularly at the level of the interspinous ligament. This damage linked to segmental instability can be diagnosed by an injection of local anesthesia into the ligament. The treatment of this pathology involves spinal manipulation. It can be associated with pain related to a minor painful intervertebral disturbance.
Low back pain and minor intervertebral pain
The pain is linked to mechanical dysfunction of a vertebral segment without a clear etiology demonstrated by imaging. It responds to treatment by manipulation (osteopathy) and can be consolidated by rehabilitation techniques.
Lumbosacral low back pain and segmental cellulo-teno-periosto-myalgia syndrome.
Always associated with other pathologies in the form of myalgic cords particularly in the gluteal muscles (myofascial syndrome of the gluteus medius for example). Sometimes these pains predominate in the painful picture and their treatment provides significant relief.
Treatment
Subscribers and doctors section