Anatomical reminder
Composed of 2 muscles: the extensor digitorum longus and the extensor hallucis longus.
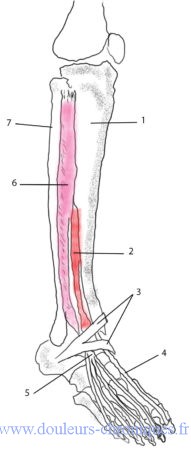
1 -Tibia
2-Extensor hallucis longus muscle
3-Inferior extensor reticunalum
4-Tendon of the extensor hallucis longus
5-Tendon of the extensor digitorum longus
6-Long extensor muscle of the toes
7-Fibula
The extensor digitorum longus takes its proximal insertion on the lateral condyle of the tibia then on the upper 3/4 of the anterior surface of the fibula, on the interosseous membrane and on the intermuscular septum which it shares with the neighboring muscles. Distally, the tendon, after crossing the superior and inferior reticunalums, divides into four and inserts on the 2nd and 3rd phalanges of the first 4 toes. The tendon then spreads out to form the extensor cap on the first phalanx and sends lateral extensions attaching to the distal phalanx.
The extensor hallucis longus takes its proximal insertion on the middle 2 quarters of the medial aspect of the fibula, its body is located between the tibia and the medial aspect of the extensor digitorum longus. At the ankle, the tendon passes deep into the superior extensor reticunalum. At its distal end, it attaches to the last phalanx of the hallux.
These two muscles help control the descent of the forefoot towards the ground after the impact of the heel on the ground during walking. During the swing phase of walking they help release the foot from the ground. The extensor digitorum longus helps to balance walking by balancing the traction of the tibialis anterior, they put the foot in dorsiflexion and eversion and, finally, it produces an extension of the toes. The extensor hallucis longus helps balance the foot when it is on the ground, it helps with dorsiflexion and inversion of the foot and, finally, it allows the extension of the hallux.
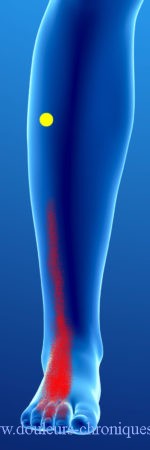
Myofascial syndrome of the extensor digitorum longus muscles
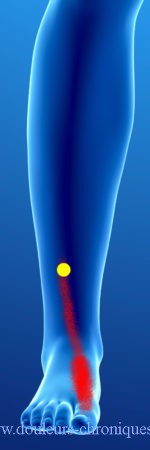
On the left, myofascial syndrome of the long extensor hallucis.
On the right, myofascial syndrome of the extensor digitorum longus.
Associated with these pains, patients may complain of weak foot dorsiflexion with a foot slamming on the ground after heel strike when walking.
These pain points can appear in:
L3-L4 root irritation
In the aftermath of falls
In case of prolonged car driving with a foot in prolonged dorsiflexion
Prolonged wearing of high heels
When jogging for too long, or walking on uneven ground for a long time
During prolonged immobilization of the ankle after trauma
the clinical examination will look for weak dorsiflexion (be careful not to miss a compression of the deep fibular nerve at the level of the proximal fibula). We find the trigger points (in yellow) on palpation of the muscles with reproduction of pain.
The treatment is done by massaging the trigger points and stretching the foot with the ankle in full extension. Of course treatment of the root cause is essential (reducing the height of shoe heels, changing the angle of a car’s accelerator pedal, decreasing the duration of jogging for some time after treatment, etc.). ..)