Anatomical reminder
From the surface to the depth we find:
–The gastrocnemius muscle composed of two heads, medial and lateral (former internal and external twin). It is inserted, proximally, on the posterior distal end of the femur and, distally, on the calcaneus by the calcaneal tendon (Achilles tendon).
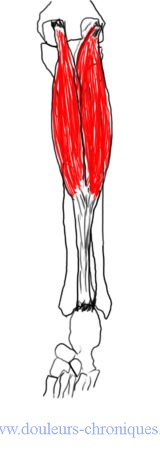
Its role is to stabilize the knee and ankle, it prevents the tibia from tilting forward. When standing and motionless it is not active. It becomes more active when the subject leans forward. It is a reserve muscle in activities such as going up or down stairs, climbing an incline, or riding a bicycle.
Its role with the soleus is to maintain posture while standing. It comes into action as soon as the position of the body in a standing position varies by more than 5 degrees.
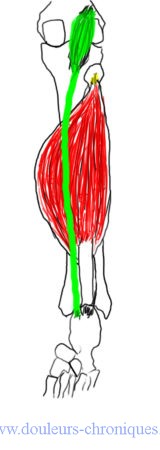
–The soleus muscle (in red) and the plantar muscle (in green).
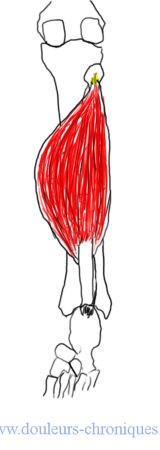
Proximal, the soleus muscle attaches to the head of the fibula and then descending along the middle third of this bone posteriorly, to the middle third of the medial aspect of the tibia and to the aponeurosis located between these 2 bones. Distally, it joins the gastrocnemius to form the Achilles tendon.
The inconstant plantaris muscle attaches proximally to the femur (distal) and has a long tendon that runs between the gastrocnemius and soleus to attach distally to the median posterior edge of the calcaneus.
The soleus stabilizes the knee and ankle when walking and limits the forward rotation of the tibia on the stationary foot. The soleus and the plantar bring the foot into plantar flexion.
–the posterior tibialis muscle and the long flexors of the toes

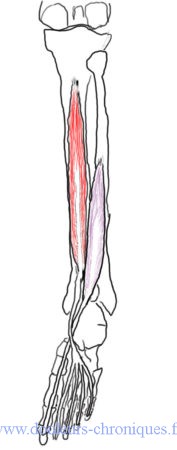
The posterior tibial muscle attaches proximally to the fibula, the tibia, the interosseous membrane. Distal, the tendon passes behind the medial malleolus and attaches to the navicular, calcaneus, cuneiforms, cuboid and 2nd, 3rd and 4th metatarsals. It acts as a supinator and maintains, by limiting pronation, the harmonious contact of the metatarsals with the ground.
The flexor digitorum longus muscle is inserted, proximally, on the middle 2/4 of the posterior surface of the tibia. The fibers converge on the tendon which passes behind the medial malleolus in a groove which it shares with the tendon of the posterior tibialis (independent synovial sheath). This tendon then crosses the superficial aspect of the flexor hallucis tendon. In the middle of the foot, the tendon splits in two and passes through the tendon of the flexor digitorum brevis to insert on the base of the last distal phalanx of the 4 toes.
The flexor hallucis longus takes its insertion on the last 2 thirds of the fibula. The muscle fibers come together to form the tendon at the posterior surface of the distal part of the tibia. The tendon then crosses the posterior surface of the talus and the lower surface of the calcaneus then it passes under the tendon of the flexor digitorum longus to insert distally on the base of the last phalanx of the hallux.
These two flexor muscles play a role in stabilizing the foot and ankle in the middle and at the end of the stance phase. They allow flexion of the last phalanges and plantar flexion when the foot is free.
Myofascial syndrome:
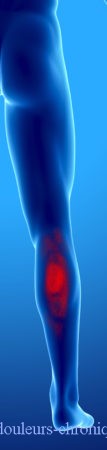
The gastrocnemius muscle:




The area responsible for the pain is in green, in red the areas of referred pain.
One of the common manifestations of gastrocnemius myofascial syndrome is calf cramps. They most often occur when the subject has remained lying down and rests the foot in prolonged plantar flexion (night awakening after several hours of sleep, for example). the treatment is done by active or passive dorsiflexion.
Another manifestation of this syndrome is intermittent claudication defined by the onset of pain after a certain distance of walking. This intermittent claudication is primarily linked to ischemia or a neurological origin. Treatment of the myofascial syndrome associated with these pathologies can improve patient performance and reduce the pain caused by the initial phenomenon.
Note that these cramps are sometimes associated with S1 radiculopathy and can be caused or aggravated by dehydration, hypomagnesemia, hypokalemia, hypocalcemia, Parkinson’s disease (dystonic form).
The activation of the myofascial syndrome is linked to repeated plantar flexion movements with the knee bent (walking on a slope, rock climbing, cycling with a saddle that is too low, walking on an inclined floor). This syndrome can be aggravated by wearing socks whose elastic is located just below the knee, wearing high heels for a long time can also promote it.
The differential diagnoses of these pains are:
– Tennis leg (muscular tear of the gastrocnemius)
– phlebitis
– a popliteal cyst
– Tendinopathy of the Achilles tendon
The treatment is done by massage and then extension of the muscles by passive dorsiflexion. In some cases the infiltration of the trigger zone with lidocaine can improve the situation always accompanied by stretching.
Corrective actions include:
– Avoid high-heeled shoes,
– Beware of a car accelerator pedal that is too hard or too flat
– Ensure correct support of the feet in a seated position.
– Avoid elastic bands that are too tight under the knee
– Avoid climbing sides on foot for too long, or walking on transversely sloping ground
– Regularly do stretching exercises at home.
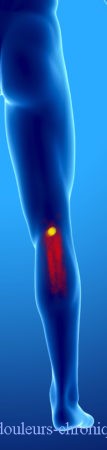
The soleus muscle:



In the diagram above the referred pain linked to the myofascial syndrome. The most frequent being point 1 described in the diagram responsible for pain in the heel and the arch of the foot.
The myofascial syndrome of the soleus is favored by walking on inclined planes, by prolonged attitudes in plantar flexion (chair too high, high heels, foot in plantar flexion during the night.
Corrective measures and treatment are similar to those for overlying gastrocnemius.
The plantar muscle:
The causes and treatment of myofascial syndrome in the plantar muscle are the same as for the soleus muscle. Note that a rare form of intermittent claudication is linked to compression of the popliteal artery by the tendon of the plantar muscle.
The posterior tibial muscle:

The pain associated with myofascial syndrome of the posterior tibialis is intense in the arch of the foot and the Achilles tendon. They occur especially when the subject walks or runs on irregular surfaces. This discomfort can appear when practicing the activities mentioned above. They can also occur when the subject has too pronounced foot pronation. Excessive pronation can be seen in mediotarsal hyperlaxity, when there is equinism in the ankle, when there is Morton’s foot.
The treatment consists in performing stretching of the muscle, patient on the belly foot outside the table, the foot is placed in dorsiflexion then in eversion.
Corrective measures are necessary in case of Morton’s foot. Running should be done on a smooth, level surface.
The long flexor muscles of the toes:

 Referred pain from these two muscles is mainly under the arch of the foot and the toes.
Referred pain from these two muscles is mainly under the arch of the foot and the toes.
Their appearance is favored by running or jogging on uneven ground, but also in case of pes cavus, Morton’s foot, mediotarsal hyperlaxity, walking with an excessively pronated foot.
The treatment is done patient on the stomach, knee at 90°, foot in dorsiflexion and extension of the toes.
Self-stretching by the patient is done with the heel on the ground with the foot in dorsiflexion with stretching and extension of the toes.
We will avoid taking shoes that are too short preventing the complete extension of the toes.
Corrective soles will also be an interesting contribution.