Pain related to the abdominal musculature often poses diagnostic problems. Indeed, the relationships with the underlying viscera are close. Thus, myofascial syndromes of the abdominal muscles can be responsible for digestive or genitourinary disorders such as colitis, heartburn, nausea, diarrhea, bladder spasms, dysmenorrhea, etc.
Similarly, visceral problems are able to trigger pain in the abdominal muscles which may persist even after the initial visceral pathology has disappeared.
Anatomical reminder:
The fibers of the two medial muscles are oriented vertically: the rectus muscle and the abdominal pyramidal muscle.

the rectus muscle

the abdominal pyramidal muscle
The lateral muscles have intersecting fibers: the external oblique muscle on the surface, the fibers of which run from top to bottom from the outside to the inside, the underlying internal oblique muscle, the fibers of which run from top to the bottom from the inside out and the deepest transverse muscle whose fibers are horizontal.
the external oblique muscle
oblique muscle
transverse muscle
Pains and symptoms:
The rectus abdominis muscle:
Symptoms largely depend on the location of the myofascial syndrome. There are three major regions giving different referred pain. The supra-umbilical upper part, the periumbilical part and the lower part (green dots).
The upper part can give back pain in bar (in yellow) associated with feelings of gastric fullness, nausea or even vomiting with epigastric pain. Pain in the upper part of the muscle can also be reminiscent of cholecystitis, gastric ulcer, pancreatitis, or even angina pectoris pain.
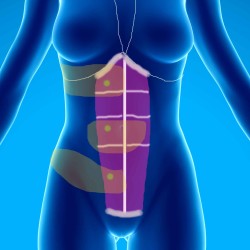

Reaching the periumbilical part of the muscle is readily responsible for sensations of intestinal spasms or colic. It can trigger diffuse abdominal pain. Patients feel the need to lean forward for relief. These pains tend to come on and get worse as the day goes on.
Involvement of the lower part may be responsible for bar pain radiating in the back towards the sacroiliac joints. They can be responsible for dysmenorrhea (anomaly of menstruation), sometimes the symptoms are those of an acute appendicitis whose particularity is to appear when the patient is tired.
The pyramidal muscle of the abdomen:
Generally responsible for isolated medial subumbilical pain.
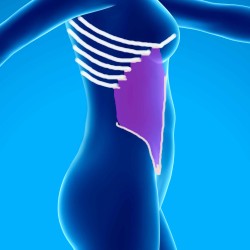
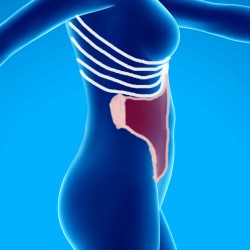
The oblique muscles of the abdomen:

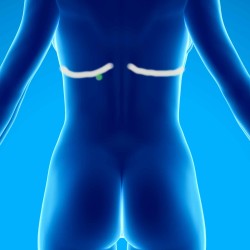
The pains coming from the external oblique (green point) in its upper part give pains referred to the level of the epigastrium (fuchsia zone) with a feeling of “deep” pain, can be associated with gastric reflux sometimes qualified of “hiatal hernia pain”.
Pain originating from the lower external oblique (green dot) radiates to the inguinal crease and external genitalia (fuchsia area). In the most medial part, the myofascial syndrome can be responsible for an irritable bladder with pain referred to the level of the bladder.
The lower part of the oblique muscles can also be responsible for diarrhea.
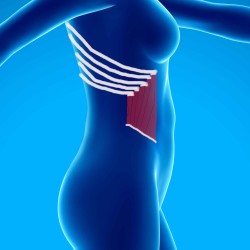
The transverse abdominis muscle:
It is responsible for pain radiating between the two sides of the costal grill, at the level of the middle part of the abdomen.
Notion of reference points:
This phenomenon is rare.
It is a dot (green dot) located under the 12th rib on the right or left in its posterior part, near the costovertebral angle.
This point is responsible for aerophagia, frequent belching or even jet vomiting.
When pressing this point, the patient emits a referral.
Treatment :
It is the same as for the other muscles:
Massage, stretching, ischemic compression.
Sometimes infiltrations of local anesthetics in the responsible areas can confirm the diagnosis and make the myofascial syndrome disappear.
Exercises are also recommended such as abdominal breathing, pelvic tilt exercises, lying down exercises, seated lying down.