Pain in breast cancer depends on the disease itself and its local and metastatic course, but also on the treatments implemented.
Cancer pain.
Pain from excess nociception.
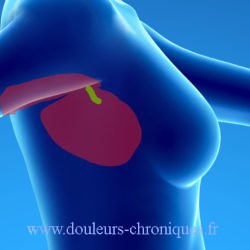
Linked to its more or less inflammatory character, its volume, its location. The pain is localized on the breast, it is rather dull, throbbing.
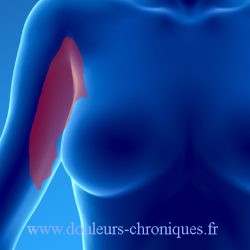
Neuropathic pain.
Related to the volume of the tumor or its location, particularly in the event of local invasion of the chest wall with damage or compression of an intercostal nerve. The localization of the pain in the 2 cases generally extends to the thoracic semi-girdle.
We find his symptomatology through the DN4 Questionnaire
Pain related to metastases.
The sites of metastases are, in order of frequency:
- Bone (more or less localized pain worsening at night relieved by the usual analgesics including NSAIDs),
- The liver (loss of appetite, nausea or disgust for certain foods, itching),
- The lung (shortness of breath, cough, hemoptysis, chest pain),
- The skin,
- The bone marrow and
- The brain (headaches, dizziness, blurred vision, tingling, numbness or weakness in the arms, hands or legs).
Some particularities are linked to the tumor profile:
- Lobular cancers metastasize to the serosa (stomach, ovaries);
- Hormone-sensitive cancers metastasize to bone (pelvis, lumbar spine, ribs, femur), lymph nodes and skin;
- Tumors lacking hormone receptors metastasize to the liver, lungs and cerebro-meninges;
- HER2-overexpressing cancers metastasize to the brain.
Pain related to breast cancer treatment.
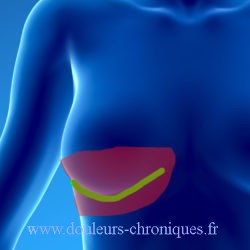
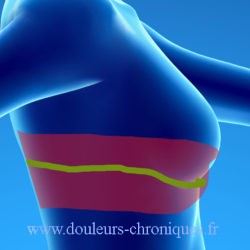
- They are usually of neuropathic origin:Cicatricial neuropathy related to tumor removal or mastectomy +/- lymph node dissection.
The characteristics of the pain are found in the DN4 questionnaire
The topography of the pain is schematized below (in green the scar, in red the painful area)..
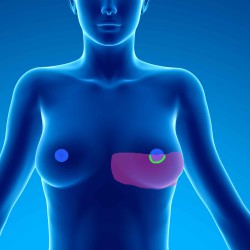
- Lymphedema of the right upper limb related to the ablation of the lymph nodes of the axillary hollow.
The upper limb is the seat of a persistent edema which can be painful. - Cicatricial neuropathy related to breast reconstruction:
The pains are also of the neuropathic type, their location depends on the techniques used.
Reconstruction techniques involve:- breast prostheses :
The location of the pain depends on the technique of fitting the prosthesis:- by peri-nipple approach

- By under the breast:
- By axillary approach:
- by peri-nipple approach
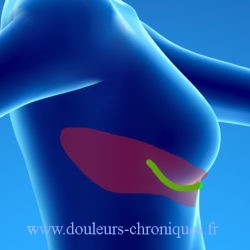
- Breast reconstruction by flaps:
- Latissimus dorsi muscle flaps (the most widely used technique at present)
Given the technique, the pain is also in the semi-girdle but its origin can come from the area where the muscle was taken:
- Latissimus dorsi muscle flaps (the most widely used technique at present)
- breast prostheses :
-
-
- The other flap reconstruction techniques (gluteus maximus, rectus abdominis, abdominal) are rarer, the painful sequelae are not listed on this site.
-
- Chemotherapy pain:
- Essentially neurological damage predominant distally and often affecting the hand and foot with burning sensation, paresthesia, electric shocks.
- gynecological damage is often present (vaginal dryness) with repercussions on intimate life.
Breast cancer pain treatment.
First of all, it will be recalled that pain concerns a patient and that pain which becomes chronic obeys a bio-psycho-social model. Treatment can therefore involve specific treatments, but sometimes psychological treatment and/or relaxation methods can be very beneficial.
Treatment of pain due to excess nociception.
It uses the usual analgesic drugs classified into 3 levels by the WHO (in link)
Treatment of neuropathic pain.
Medical treatment :
These are treatments that are taken daily and which, unfortunately, are not without side effects. They are sometimes little, see ineffective.
Antidepressant drugs:
- Laroxyl (amitriptyline),
- Anafranil (clomipramine),
- Effexor (venlafaxine),
- Cymbalta (duloxetine),
- Ixel (milnacipran).
Antiepileptic drugs:
- Neurontin (Gabapentin),
- Lyrica (pregabalin),
- Trileptal (oxcarbazepine),
- Tegretol (carbamazepine).
Local treatments for scarring neuropathic pain.
- Subscar injection of lidocaine (unpublished)
- Application of capsaiscin (Qutenza) on the affected areas (if effective, effectiveness of several weeks to renew regularly)
- Application of local anesthetic plaster (Versatis) (adjunctive treatment no more than 12 hours a day)
- Botulinum toxin injection (technique under development in some centers)
Treatment of chemotherapy sequelae.
Pain can be treated with general medication,
They may also respond to the application of capsaicin (Qutenza).
In the particular case of gynecological damage, the use of local laser treatment seems particularly effective (vaginal dryness).
Treatment of metastatic pain.
The different types of treatment generally available will be used.
In the particular case of bone metastases:
- NSAIDs are particularly effective on this type of pain
- Radiation therapy is also effective
- In some cases local cementoplasty techniques are used (Spine, pelvis)